If you’re preparing for the United States Medical Licensing Examination® (USMLE®) Step 1 exam, you might want to know which questions are most often missed by test-prep takers. Check out this example from Kaplan Medical, and read an expert explanation of the answer. Also check out all posts in this series.
This month’s stumper
A 60-year-old man comes to the physician because of tender blisters on his arm and flank, worsening over the last few months. His medical history includes hypertension and hyperlipidemia. He is taking atorvastatin and hydrochlorothiazide for these conditions. Physical examination shows blisters and flaccid bullae; a few have ruptured, leaving red, sore, denuded areas. Pathologic examination reveals acantholysis and few lymphocytes.
Which of the following findings is most likely in this patient?
A. Eosinophils within bullae.
B. IgA deposits in the dermal papillae.
C. IgG antibody against hemi-desmosomes.
D. Negative Nikolsky sign.
E. Oral mucosal lesions.
The correct answer is E.
Kaplan Medical explains why
Pemphigus vulgaris (PV) is a rare and potentially fatal autoimmune condition seen in middle-aged to older adults. It is associated with painful, flaccid suprabasal/intraepidermal bullae formation on the skin and oral mucosa.
The condition results from formation of IgG directed against epithelial desmosome protein (desmoglein 3), resulting in intraepidermal keratinocyte separation (acantholysis) and bullae formation. The flaccid bullae in this disease reflect the poor cell-to-cell adhesion between keratinocytes due to desmosome dysfunction. The bullae also present with a positive Nikolsky sign, in which manual stroking of these blisters results in their rupture. Ruptured bullae leave red, raw areas, which can mimic burns. If not treated with steroids, most patients will die within one year.
The statin and hydrochlorothiazide did not contribute to PV. Medication-induced PV is rare, but can be caused by antipsychotics, spironolactone, or sulfonamides, and usually presents with cutaneous lesions without involvement of the oral cavity.
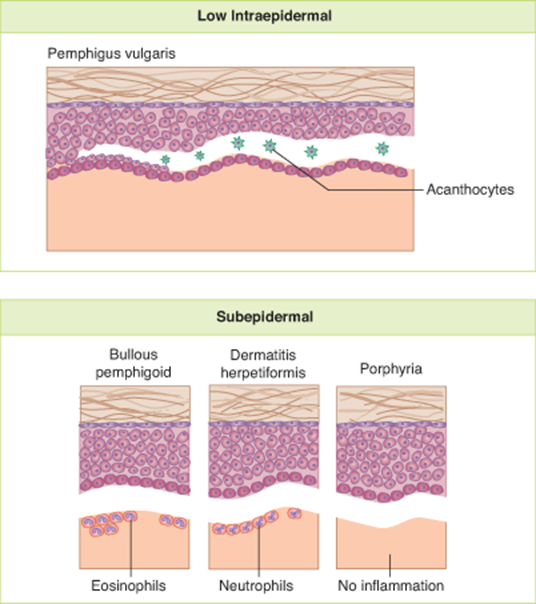
The figure below compares the types of blisters.
Why the other answers are wrong
Choice A and C: An important condition on the differential diagnosis for autoimmune blistering conditions is bullous pemphigoid (BP). Histologically, prominent eosinophils within blisters would support bullous pemphigoid as the diagnosis. This condition presents with IgG autoantibodies against hemidesmosomes. Hemidesmosomes anchor basal keratinocytes to the basement membrane. As a result, the epithelial layer lifts off the basement membrane producing a non-flaccid, tense sub-epidermal/sub-basal blister.
Subscribe and succeed in medical school
Get tips and insider advice from the AMA on succeeding in medical school—delivered to your inbox.

Unlike pemphigus vulgaris, bullous pemphigoid does not affect desmosome adhesion proteins. The associated antigens are: bullous pemphigoid antigen 1 and 2 (BPAG1, BPAG2). Patients with BP usually present with pruritus in the skin surrounding the blister rather than pain. Bullous pemphigoid can affect various areas of the skin but mucosal involvement is uncommon, unlike pemphigus. Pemphigoid also has a more favorable prognosis.
Choice B: IgA deposits in the dermal papillae is characteristic of dermatitis herpetiformis. Patients present with pruritic vesicles and papules at the dermal-epidermal junction, primarily on extensor surfaces. The disease is strongly associated with gluten sensitivity and celiac disease, and may result from cross-reactivity between gluten and reticulin in the epidermal basement membrane.
Choice D: Blisters that are resistant to shear stress and do not readily rupture present with a negative Nikolsky sign. This negative sign is seen with subepidermal blisters such as bullous pemphigoid, dermatitis herpetiformis, and porphyria cutanea tarda. It is worth a brief mention of porphyria cutanea tarda, the most common form of porphyria.
It has an autosomal dominant inheritance pattern and is characterized by a defect in uroporphyrinogen decarboxylase (part of heme synthesis). Patients present with painful, small, subepidermal photosensitive blisters on sun-exposed skin (face, hands, arms and legs) due to buildup of porphyrin compounds close to the skin.
Tips to remember
- Pemphigus vulgaris is a rare condition seen in middle- to older-aged adults.
- It is associated with painful flaccid supra-basal/intraepidermal bullae formation on the skin and oral mucosa.
- Other features include IgG antibodies against desmosomes and a positive Nikolsky sign.
For more prep questions on USMLE Steps 1, 2 and 3, view other posts in this series.
The AMA and Kaplan have teamed up to support you in reaching your goal of passing the USMLE® or COMLEX-USA®. If you're looking for additional resources, Kaplan provides free access to tools for pre-clinical studies, including Kaplan’s Lecture Notes series, Integrated Vignettes, Shelf Prep and more.



